Bone Densitometry Techs’ Role in Osteoporosis Screening

- Understanding Osteoporosis: The Basics
- Key Risk Factors
- Signs and Symptoms
- Official Recommendations and Guidelines: Empowering Your Practice
- American College of Radiology (ACR) Recommendations
- US Department of Health and Human Services Recommendations
- The Radiologic Technologist’s Indispensable Role
- Patient Education and Screening
- Optimal Image Acquisition
- Recognizing Incidental Findings
- Communication with Radiologists
- Quality Assurance and Patient Safety
- Conclusion
- References
Osteoporosis is a common skeletal disorder that reduces bone mineral density and bone mass, or when the quality or structure of the bone changes. Osteoporosis is also known as a silent killer, because it does not have noticeable symptoms until the bone breaks. In the United States, osteoporosis is linked to approximately 3 million fractures in the year 2025, particularly in postmenopausal women and older adults, and often goes undiagnosed until a fracture occurs.
Bone densitometry technologists and radiologic technologists play a vital role in identifying osteoporosis, monitoring its progression, monitoring treatment responses, and assessing related fractures. Their hands-on experience with this disease and imaging expertise contribute to spreading awareness and management.
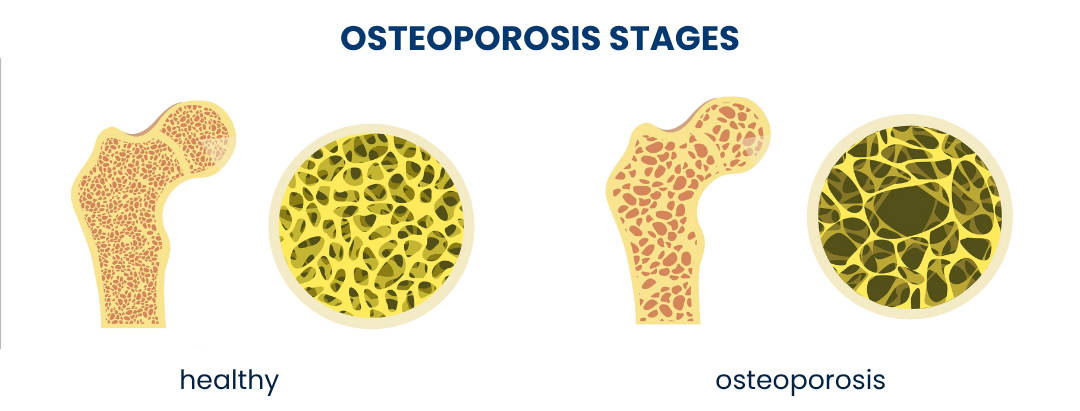
Understanding Osteoporosis: The Basics
In healthy individuals, the process of bone resorption (the breakdown of old bones) and the process of bone formation (the building of new bones) remain in balance. Osteoporosis interferes with this natural balance where resorption exceeds formation, leading to the presence of porous and weakened bones, making them more susceptible to fractures. Understanding this imbalance and detecting it before fractures occur is the key to managing osteoporosis effectively.
In 2024, 10 million Americans over the age of 50 are living with osteoporosis, according to the Office of the Assistant Secretary for Health (OASH). An additional 44 million have low bone density, which makes them vulnerable to an increased risk of osteopenia. The CDC projects that this number will increase by over 30% by 2030, underlining the urgent need for spreading awareness on early screening and prevention strategies.
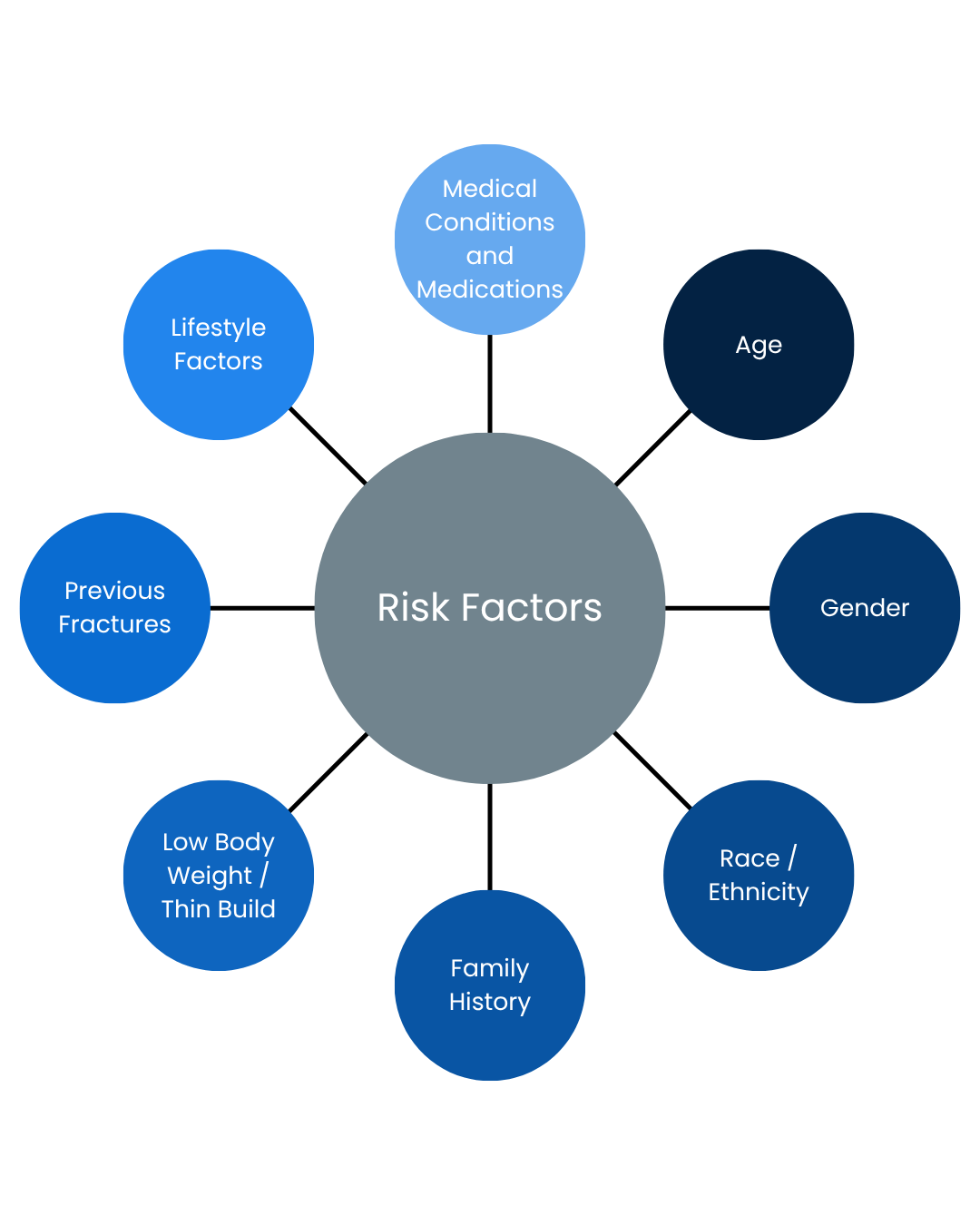
Key Risk Factors:
Several factors contribute to an individual’s risk of developing osteoporosis. These include:
- Age: The risk increases significantly with advancing age.
- Gender: Women are at a higher risk, especially after menopause, due to declining estrogen levels.
- Race/Ethnicity: Non-Hispanic white and Asian individuals have a higher predisposition.
- Family History: A parental history of hip fracture or osteoporosis increases risk.
- Low Body Weight/Thin Build: Individuals with a smaller, thinner frame may have less bone mass to begin with.
- Previous Fractures: A history of fragility fractures (fractures from minor trauma) is a strong indicator.
- Lifestyle Factors: Smoking, excessive alcohol consumption, sedentary lifestyle, and inadequate intake of calcium and vitamin D.
- Medical Conditions and Medications: Certain chronic diseases (e.g., rheumatoid arthritis, celiac disease, chronic kidney disease) and medications (e.g., glucocorticoids, certain cancer treatments) can hurt bone health.

Signs and Symptoms
Osteoporosis typically progresses silently, without identifiable symptoms in its early stages. As bone density decreases, patients may remain unaware of their condition until a fragility fracture occurs, often from a low-impact accident such as a minor fall, bending, or even coughing.
Fractures occurring in the spine (vertebrae), hip, wrist, and forearm are often the first clinical sign of advanced bone loss. One of the most common and debilitating consequences is the spinal compression fracture, which can lead to:
- Chronic back pain
- A gradual loss of height
- A stooped posture, known as a dowager’s hump

These changes result from the collapse of weakened vertebral bodies, affecting both mobility and quality of life. In severe cases, especially after a hip fracture, osteoporosis can even contribute to increased mortality.
Other subtle indicators of bone loss may include:
- Receding gums (linked to jawbone loss)
- Decreased grip strength
- Brittle or ridged fingernails
While these signs are less specific, they should prompt further evaluation when risk factors are present.
The Gold Standard: DXA and Imaging Modalities
For accurate diagnosis and monitoring of osteoporosis, Dual-energy X-ray Absorptiometry (DXA) is the widely accepted gold standard. DXA utilizes low-dose X-rays to measure bone mineral density (BMD) at clinically significant sites (such as the lumbar spine and hip). The results are expressed as a T-score, which compares the patient’s BMD to that of a healthy young adult reference population:
- T-score ≥ -1.0: Normal bone density
- T-score between -1.0 and -2.5: Osteopenia (low bone mass)
- T-score ≤ -2.5: Osteoporosis
While DXA remains the cornerstone for osteoporosis diagnosis, alternative imaging modalities may be needed in certain clinical situations, such as when DXA results are inconclusive, anatomical challenges exist, or fractures are suspected without prior BMD assessment.
- Vertebral Fracture Assessment (VFA): Often performed alongside DXA, VFA is a low-radiation technique that uses additional software to analyze images of the thoracic and lumbar spine. VFA employs lateral spine imaging to detect vertebral compression fractures. These fractures are strong predictors of future osteoporotic injury, even in the absence of a formal osteoporosis diagnosis.

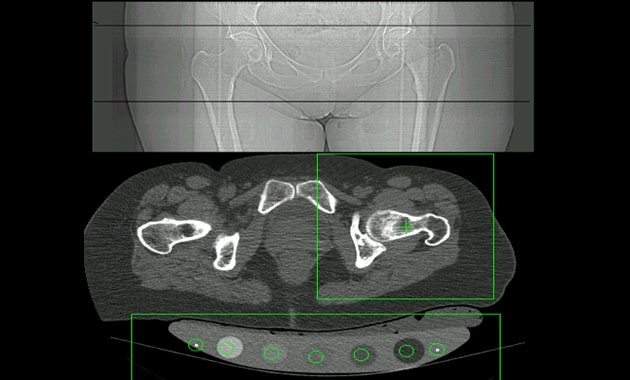
Quantitative Computed Tomography (QCT): QCT is a 3D medical imaging technique that uses routine CT scanning with a calibration standard to measure bone mineral density. Though it involves higher radiation exposure, QCT offers volumetric BMD measurements and distinguishes between cortical and trabecular bone. It’s mostly useful in complex cases or when degenerative changes might falsely elevate DXA readings.
Radiography: Standard X-rays are not sensitive enough for early osteoporosis diagnosis (requiring ~30% bone loss to be visible) but are crucial for identifying fractures and excluding other causes of bone pain.
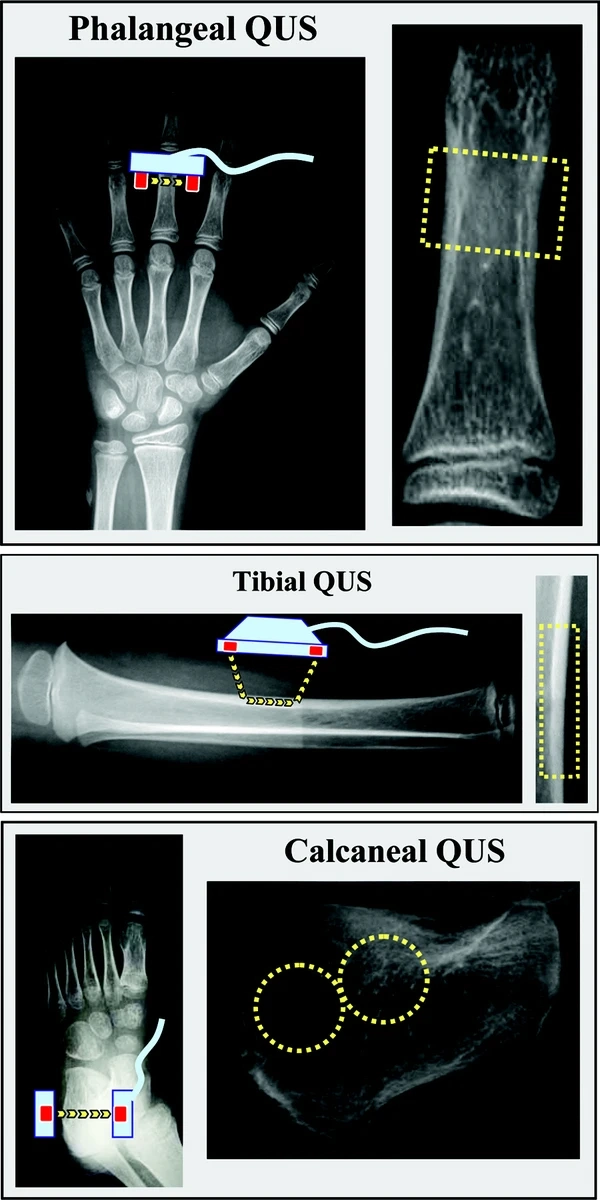
- Quantitative Ultrasound (QUS): QUS provides a radiation-free screening option commonly used at peripheral sites such as the heel (calcaneus). While not diagnostic and not endorsed as a standalone tool by ACR or WHO, it is valuable for initial risk assessment, particularly in primary care settings. Abnormal findings on QUS often warrant follow-up with DXA.
Official Recommendations and Guidelines: Empowering Your Practice
American College of Radiology (ACR) Recommendations:
- The role of the ACR is crucial in establishing imaging guidelines for various clinical conditions, including osteoporosis. The ACR Appropriateness Criteria® Osteoporosis and Bone Mineral Density are evidence-based guidelines that inform the appropriate use of imaging modalities.
Key recommendations for BMD testing generally include:
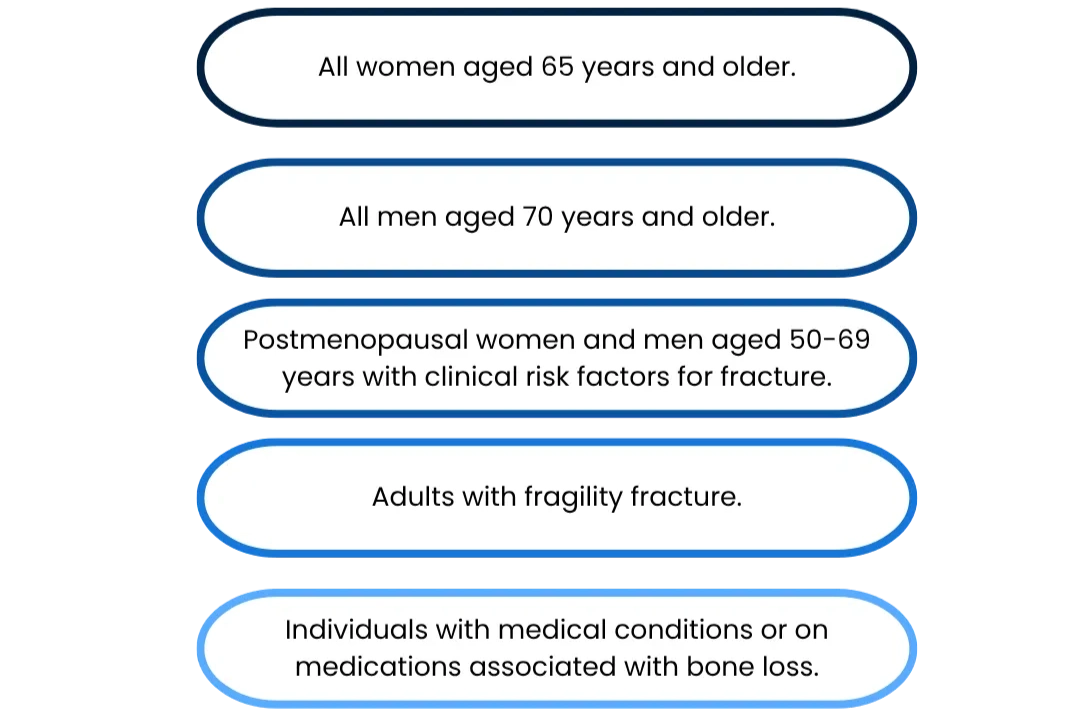
For detailed and updated guidelines, please refer to the official ACR website: https://www.acr.org/ (navigate to Appropriateness Criteria and search for Osteoporosis and Bone Mineral Density).
U.S. Department of Health and Human Services Recommendations
Various agencies within the U.S. Department of Health and Human Services, such as the Office on Women’s Health and the National Institute on Aging, provide comprehensive guidance on osteoporosis prevention, diagnosis, and treatment for the public. These recommendations emphasize:
- Adequate Calcium and Vitamin D Intake: Essential nutrients for bone health, often requiring dietary adjustments or supplementation
- Regular Weight-Bearing Exercise: Activities like walking, jogging, lifting weights, and dancing help build and maintain bone density
- Smoking Cessation and Moderate Alcohol Consumption: Both smoking and excessive alcohol intake negatively impact bone health.
- Fall Prevention Strategies: Crucial for individuals with osteoporosis to minimize fracture risk.

For reliable information and resources on osteoporosis care and support clinics, visit the following official links:
- Office on Women’s Health: womenshealth.gov
- National Institute on Aging: www.nia.nih.gov
The Radiologic Technologist’s Indispensable Role
As a radiologic technologist, your contribution to osteoporosis detection and prevention extends well beyond operating the DXA scanner. Your expertise and patient-facing role place you in a pivotal position to influence early intervention and ensure diagnostic accuracy.
1. Patient Education and Screening: You are often the first point of contact during imaging, making you uniquely positioned to:
- Identify at-risk individuals: Stay alert to common risk factors such as age, gender, family history, and previous fractures during patient intake and preparation.
- Provide basic education: Help patients understand what osteoporosis is, its silent nature, and why screening matters. Even brief conversations can prompt patients to discuss bone health with their referring providers.
- Explain the DXA procedure: Alleviate anxiety by clearly communicating the scan’s purpose, safety, and non-invasive nature, especially for first-time patients

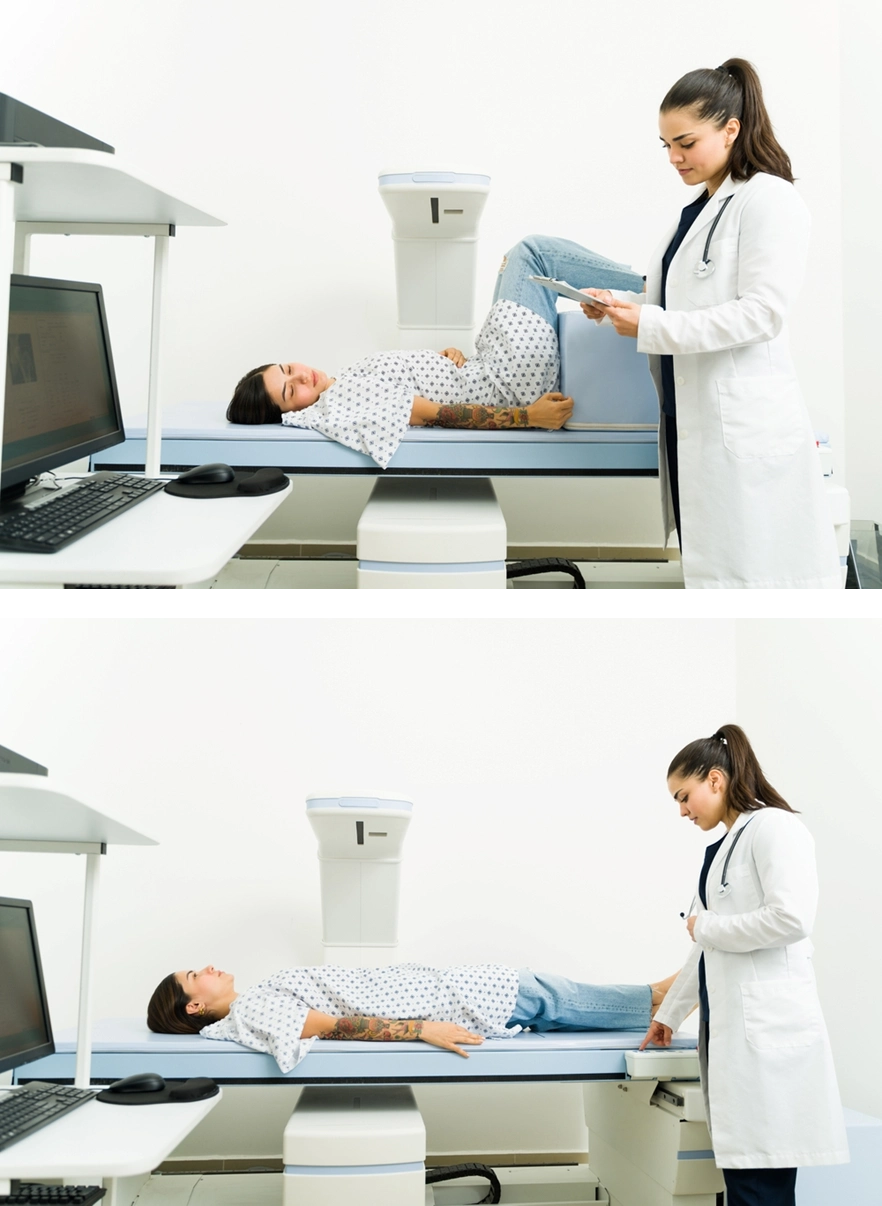
2. Optimal Image Acquisition: Accurate DXA results depend on meticulous imaging techniques. Your responsibilities include:
- Correct patient positioning: Follow standardized protocols for spine, hip, and forearm positioning to ensure valid and reproducible BMD measurements.
- Proper equipment calibration and quality control: Perform regular checks on DXA equipment to maintain accuracy and comply with accreditation standards.
- Artifact recognition and avoidance: Identify and mitigate common image artifacts or external factors (e.g., clothing, motion, surgical implants) that may skew results.

3. Recognizing Incidental Findings: Even when performing non-DXA studies like radiographs or CT scans, you may encounter subtle signs of low bone density. Stay vigilant for:
- Vertebral compression fractures: Often visible as wedge-shaped or biconcave deformities on lateral spine radiographs.
- Generalized osteopenia: A diffuse reduction in bone density across imaging studies.
- Cortical thinning: Noticeably reduced outer bone layers.
- Increased trabecular prominence: More apparent bone struts due to loss of surrounding material.
These findings, while not diagnostic on their own, should be formally documented and communicated to the interpreting radiologist, along with a suggestion for a DXA referral if appropriate.
4. Communication with Radiologists: Clear, timely communication is essential. Notify radiologists of any findings suggestive of osteoporosis or incidental abnormalities. Your collaboration ensures that important indicators of bone loss are not overlooked, facilitating appropriate clinical follow-up.
5. Quality Assurance and Patient Safety: Uphold the highest standards of radiation safety, especially when performing DXA scans that use minimal radiation doses. Apply the ALARA (As Low As Reasonably Achievable) principle consistently to protect patients while ensuring diagnostic quality. Your adherence to safety protocols fosters trust and reinforces your role as a guardian of imaging quality and patient well-being.
Conclusion
Osteoporosis is a significant public health challenge, but one that can be effectively addressed through early detection, proactive prevention, and interdisciplinary collaboration. As integral members of the radiology team, radiologic technologists possess the knowledge, skills, and unique vantage point to make a lasting impact on patient outcomes. By actively contributing to osteoporosis awareness, early screening, precise imaging, and patient education, you help reduce the burden of osteoporotic fractures and improve long-term bone health. As imaging technologies and clinical guidelines continue to evolve, your role will remain essential in shaping a proactive, patient-centered approach to bone health. Together, we can make a visible difference in the fight against this “silent” disease.
References
- womenshealth.gov
- www.nia.nih.gov
- Quantitative Computed Tomography (QCT) Radiology.ucsf.edu
- www.cdc.gov
- Quantitative Ultrasound Methods to Assess Bone Mineral Status in Children: Technical Characteristics, Performance, and Clinical Application www.nature.com
- www.gehealthcare.com
- www.hhs.gov
Disclaimer: The information provided on this website is intended to provide useful information to radiologic technologists. This information should not replace information provided by state, federal, or professional regulatory and authoritative bodies in the radiological technology industry. While Medical Professionals strives to always provide up-to-date and accurate information, laws, regulations, statutes, rules, and requirements may vary from one state to another and may change. Use of this information is entirely voluntary, and users should always refer to official regulatory bodies before acting on information. Users assume the entire risk as to the results of using the information provided, and in no event shall Medical Professionals be held liable for any direct, consequential, incidental or indirect damages suffered in the course of using the information provided. Medical Professionals hereby disclaims any responsibility for the consequences of any action(s) taken by any user as a result of using the information provided. Users hereby agree not to take action against, or seek to hold, or hold liable, Medical Professionals for the user’s use of the information provided.