Contrast-Enhanced Mammography: The Role of This New Technique


Step-by-Step Path to Certification
- How does the normal digital mammogram differ from a CEM study?
- Who can have a CEM study?
- How is the exam performed?
- Benefits of the CEM study
Contrast-enhanced mammography (CEM) is an emerging breast imaging modality that helps improve diagnostic accuracy when routine breast exams produce inconclusive findings. Contrast-enhanced mammography (CEM) uses IV injection of a dye containing iodine (used in CT) in combination with a standard digital mammogram. Unlike a standard mammography exam, dense breast tissue is not a problem in the detection of cancers. It may also serve as an alternative to breast MRI in patients unable to have one.

Contrast used for injection in a CEM study
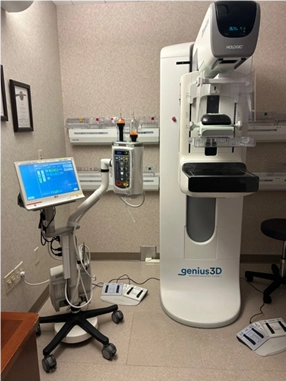
CEM study room setup
How does the normal digital mammogram differ from a CEM study?
A full field digital (FFD) 2D mammogram is the gold standard for screening patients for breast cancer. Digital breast tomosynthesis (DBT) is the newest exam in mammography for screening all patients, but especially for dense-breasted patients. A 2D mammogram is similar to taking a picture of the sky with clouds. There could be many clouds, so the sky is obstructed from view, or there could be patchy clouds where you get a glimpse of blue now and then between the clouds. Dense breast tissue is like the clouds. Some women have many glandular “clouds” in their breasts, while others may have very few. Just as we describe a beautiful day as usually having no clouds in the sky, an easy-to-read mammogram would be one without any glandular tissue in the image. The glandular tissue obstructs the radiologist from fully evaluating the breast. While a DBT exam is very helpful by creating 1 mm thick slices through the tissue to better evaluate the breast, it doesn’t completely remove the dense tissue to see the remaining surrounding tissue for proper evaluation. This is the biggest obstacle in breast imaging.
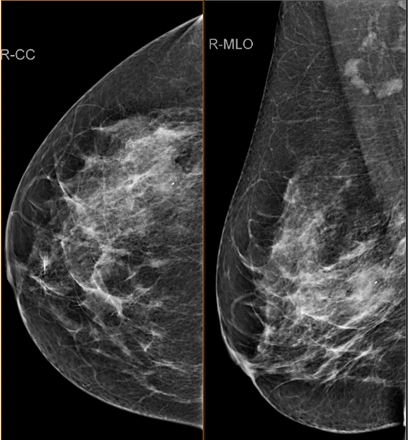
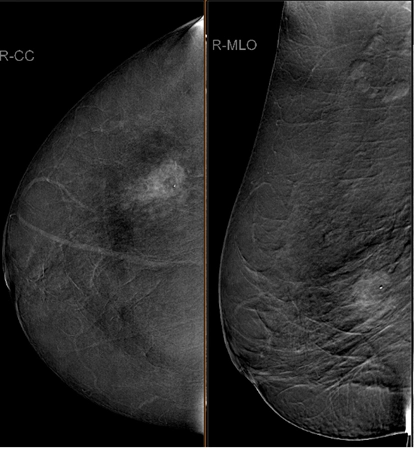
2D mammogram and CEM study showing how a dense mass can be hidden by the dense tissue in a mammogram.
Who can have a CEM study?
A contrast-enhanced mammogram (CEM) can do this! While it is still a mammogram and it does have some downfalls, the main goal of removing the dense tissue from the image for proper whole breast evaluation for breast cancer is possible with an injection of contrast before the standard mammogram is exposed. Of course, you must also have the software to perform this exam purchased separately from your manufacturer. All four FDA-approved DBT vendors in the United States have these software capabilities.
A patient must have an order from their primary care physician for a mammogram with and without contrast. At this time, it is FDA-approved only as a diagnostic exam. Therefore, a patient cannot request this exam on their own. The FDA approved the exam to visualize breast lesions in adults when standard mammograms are inconclusive or when further evaluation is needed, especially for women with dense breasts.
- CEM combines standard digital mammography with an IV injection of an iodine-based contrast agent.
- The contrast dye highlights areas of abnormal blood vessels or hyperactive tissues, which can be signs of cancer.
- This technique provides additional functional information about breast tissues,similar to breast MRI, allowing for better visualization of abnormalities.
Fig. 1. What does a CEM study show?
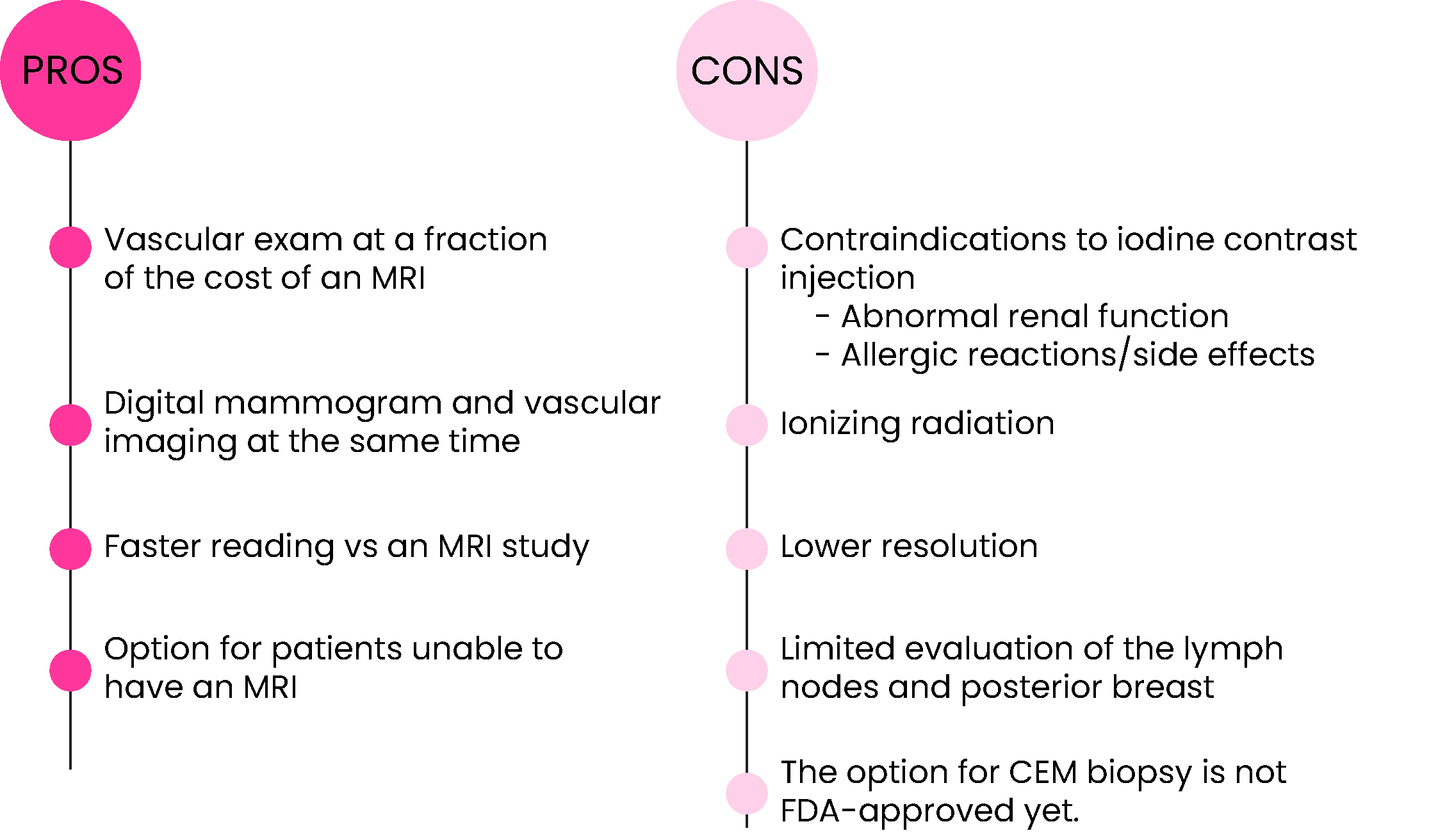
Pros
- Vascular exam at a fraction of the cost of an MRI
- Digital mammogram and vascular imaging at the same time
- Faster reading vs an MRI study
- Option for patients unable to have an MRI
Cons
- Contraindications to iodine contrast injection
- Abnormal renal function
- Allergic reactions/side effects
- Ionizing radiation
- Lower resolution
- Limited evaluation of the lymph nodes and posterior breast
- The option for CEM biopsy is not FDA-approved yet.
How is the exam performed?
First, an IV is placed into the patient’s vein for injection of the iodine-based contrast. While the contrast is being injected, the patient may feel a slightly warm sensation and or get a metallic taste in their mouth. They may also feel a sensation as if they need to urinate. These are all normal reactions. 1.5 to 2 minutes after the contrast has been injected, images must begin and be taken within approximately 7-10 minutes. For each breast, there will be two mammographic images taken in the CC and the MLO views. There are four images positioned and taken, but eight images total with a CEM study. One exposure uses low-energy X-rays and looks like the standard digital mammogram. The second exposure uses higher-energy X-rays that absorb the iodine in the contrast agent. The low and high-energy images are processed by the CEM software and create an iodine-only image that shows only findings that are enhanced with the injected contrast. The dense tissue will have been subtracted out. These images will be reviewed with the low-energy standard mammogram (2D or 3D) images for diagnosis.

Patient seated while the mammography technologist is injecting the contrast.

Right MLO CEM image
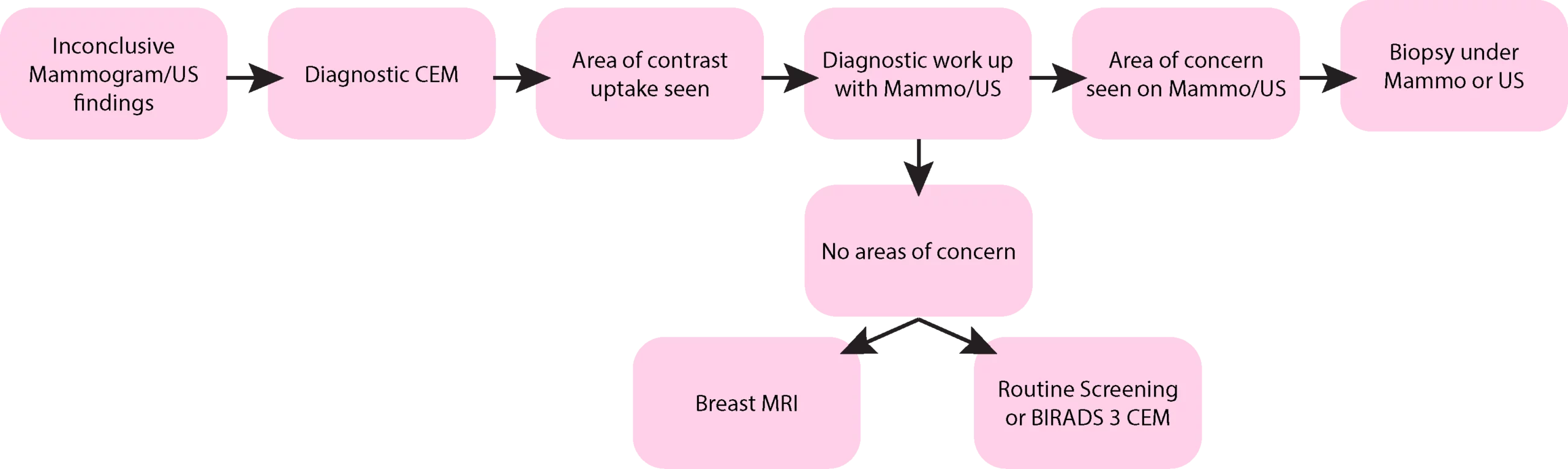
Fig. 2. Patient Flow Chart for Diagnostic CEM imaging
A typical patient work-up is seen in Fig. 2. If a diagnostic mammogram and ultrasound are inconclusive and the radiologist is looking for another modality that is inexpensive compared to an MRI, a diagnostic CEM can be ordered and performed. If the CEM study does not have any suspicious areas of uptake, then, depending on how concerned the radiologist is, the patient can go back to a routine screening mammogram the following year, or they could do a short-term follow-up (BIRADS 3) repeat contrast-enhanced study. If the radiologist is still concerned after the negative CEM study, they can send the patient for a breast MRI. If the diagnostic CEM study does show suspicious areas of contrast uptake, then the patient would return to the breast imaging area for a diagnostic mammogram and or ultrasound. If the suspicious areas are seen under mammography or ultrasound, then the patient could be scheduled for a biopsy under the corresponding modality. If there are no suspicious areas on the additional diagnostic workup up the radiologist has the option of sending the patient back to routine screening the following year or a short-term follow-up of the contrast-enhanced study. The radiologist always has the option of sending the patient for a full breast MRI exam, even with a negative diagnostic workup of the mammogram, ultrasound, and CEM studies.
Benefits of the CEM study
As predicted, a CEM study has a higher detection rate than a non-contrast mammogram, but more interestingly showed a similar detection rate with a contrast-enhanced MRI study. A study done by Memorial Sloan Kettering had 52 patients with an equal sensitivity rate between CEM and MRI. Both modalities successfully diagnosed 50 out of 52 patients. Of important note, the other two were diagnosed with ductal carcinoma in situ, and CEM and MRI are not the best modalities for the diagnosis of early breast cancers manifesting from calcifications. Other benefits are the cost to patients, the reduced time of the exam, and claustrophobia is no longer an issue.
Conclusion
CEM is a promising exam with many encouraging clinical studies performed and currently in progress. It has the potential to reduce the number of unnecessary biopsies, help with preoperative planning for the extent of disease in the breast, and be used as a modality where MRI is not an option. CEM may also be useful as a screening tool in the future. Currently, there are studies in progress to assess this possibility. High-risk patients with a history of breast cancer, or patients with dense breast tissue, potentially could be able to elect to have a screening CEM study annually, along with the guidance of their primary care physician. The one barrier to CEM becoming a widespread exam is the inability to perform a CEM-guided biopsy. Although there is a development of prototypes underway currently.
References:
Disclaimer: The information provided on this website is intended to provide useful information to radiologic technologists. This information should not replace information provided by state, federal, or professional regulatory and authoritative bodies in the radiological technology industry. While Medical Professionals strives to always provide up-to-date and accurate information, laws, regulations, statutes, rules, and requirements may vary from one state to another and may change. Use of this information is entirely voluntary, and users should always refer to official regulatory bodies before acting on information. Users assume the entire risk as to the results of using the information provided, and in no event shall Medical Professionals be held liable for any direct, consequential, incidental or indirect damages suffered in the course of using the information provided. Medical Professionals hereby disclaims any responsibility for the consequences of any action(s) taken by any user as a result of using the information provided. Users hereby agree not to take action against, or seek to hold, or hold liable, Medical Professionals for the user’s use of the information provided.