The Evolution of CT Scan: Key Developments Over the Decades



The Evolution of CT Scan Imaging: Key Developments Over the Decades
- Introduction
- Early History and Inception of CT
- The Beginning
- Generational Advances in CT Technology
- First Generation
- Second Generation
- Third Generation
- Fourth Generation
- Helical (Spiral) CT
- Multidetector CT (MDCT)
- Radiation Dose Awareness and Reduction
- Spectral (Dual-Energy) CT
- Artificial Intelligence and Deep Learning in CT Imaging
- Conclusion
- References
Introduction
Computed tomography imaging, or CT scan, commonly referred to as a CT, has become a widely used radiological exam. So, what is computed tomography? And how is it used in medical imaging?
This advanced type of X-ray examination, in which a rotating beam captures multiple images around a specific body part, is then processed by a computer to create detailed cross-sectional images. Unlike conventional X-rays, CT scans eliminate the overlap of structures by providing clear, layered views of the body, offering significantly more precise anatomical detail.
CT imaging plays a pivotal role in modern medical diagnostics due to its high diagnostic accuracy, rapid acquisition time, and advanced post-processing capabilities. Its ability to quickly generate detailed cross-sectional and three-dimensional reconstructions enhances anatomical visualization, facilitates early disease detection, and improves surgical and interventional planning. The speed and precision of CT make it indispensable in emergency settings, oncology, cardiovascular imaging, and trauma assessment, significantly contributing to improved patient outcomes.

The purpose of this paper is to trace the major milestones and innovations in CT imaging, highlighting its evolution from a groundbreaking diagnostic tool to the cornerstone of medical practice today. It will explore key technological advancements, their clinical relevance, and how these developments have enhanced diagnostic precision and patient care. Additionally, the paper will look at current trends and future directions in computed tomography imaging, emphasizing its ongoing impact on clinical decision-making and medical innovation.
Early History and Inception of the CT Scan
Before the advent of CT imaging, conventional X-rays had several key limitations that impacted diagnostic accuracy:
- Superimposition of Structures: X-rays produce two-dimensional images, resulting in overlapping anatomical structures that can obscure pathology or make localization difficult.
- Limited Contrast Resolution: X-rays are less effective at distinguishing between soft tissues with similar densities, such as the brain, liver, or abdominal organs, making subtle lesions or abnormalities hard to detect.
- Poor Spatial Localization: It was challenging to determine the exact depth or precise location of a lesion within the body using standard radiographs.
- Inadequate Visualization of Complex Anatomy: Regions like the brain, spine, and joints were difficult to assess in detail, especially for early-stage disease or trauma.
- Limited Use in Acute or Complex Cases: In emergency and trauma settings, X-rays often provide insufficient information for timely and accurate diagnosis.
These limitations highlighted the need for cross-sectional imaging, leading to the development of computed tomography. This marked a major milestone in CT scan history.
The Beginning
The first CT scanner was developed by Sir Godfrey Hounsfield, an electrical engineer at EMI Laboratories (Electrical and Musical Industries) in the United Kingdom. Working in the late 1960s, Hounsfield pioneered the technology and introduced the first head-only computed tomography scanner in 1971. Designed exclusively for brain imaging, the head-only scanner was the result of collaborative work between engineer Godfrey Hounsfield and radiologist James Ambrose.
 Godfrey Hounsfield -developed the first CT scan as an electrical engineer in the 1970s. https://litfl.com
Godfrey Hounsfield -developed the first CT scan as an electrical engineer in the 1970s. https://litfl.com This early system acquired a single slice over several minutes using a rotate-translate motion, followed by hours of computer processing to reconstruct the image. Despite its limitations in speed and coverage, the EMI scanner demonstrated the profound diagnostic potential of cross-sectional imaging, particularly for detecting intracranial pathology such as tumors and hemorrhages, laying the foundation for the widespread adoption of CT technology.
Independently and around the same time, Allan Cormack, a physicist in the United States, had also developed the theoretical foundations for tomographic image reconstruction.
For their contributions, Hounsfield and Cormack shared the Nobel Prize in Physiology or Medicine in 1979. Hounsfield is credited with building and demonstrating the first practical CT scanner, while Cormack provided the mathematical framework that made the technology possible.
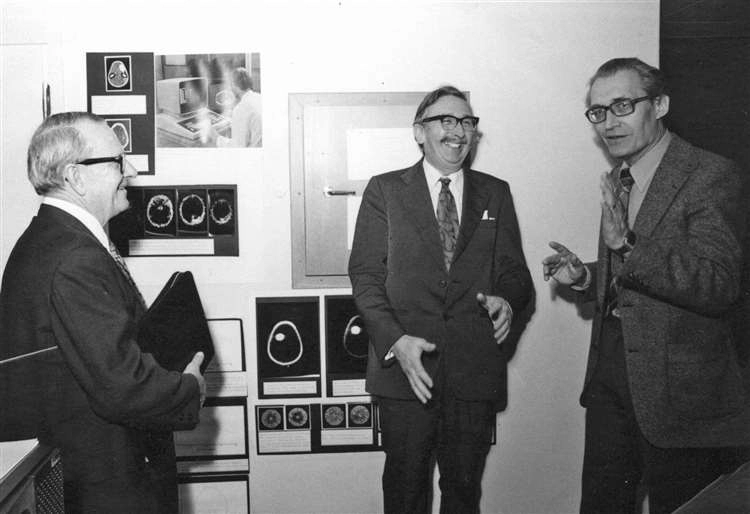 Allan MacLeod Cormack (left) and Godfrey Hounsfield with Professor Torgny Greitz (right), of the Karolinska Medico-Chirurgical Institute, in December 1979. www.johnogroat-journal.co.uk
Allan MacLeod Cormack (left) and Godfrey Hounsfield with Professor Torgny Greitz (right), of the Karolinska Medico-Chirurgical Institute, in December 1979. www.johnogroat-journal.co.uk 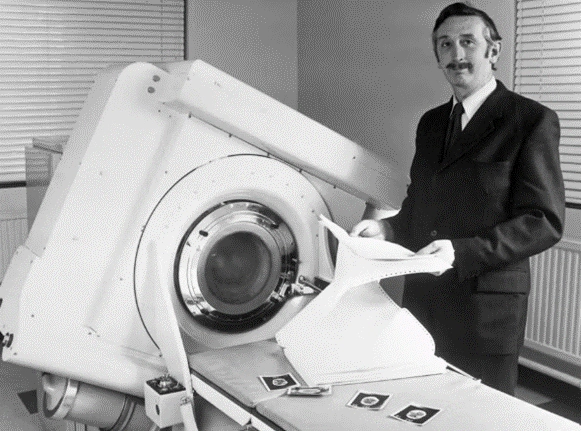 Allan MacLeod Cormack (left) and Godfrey Hounsfield with Professor Torgny Greitz (right), of the Karolinska Medico-Chirurgical Institute, in December 1979. www.johnogroat-journal.co.uk
Allan MacLeod Cormack (left) and Godfrey Hounsfield with Professor Torgny Greitz (right), of the Karolinska Medico-Chirurgical Institute, in December 1979. www.johnogroat-journal.co.uk Generational Advances in CT Technology
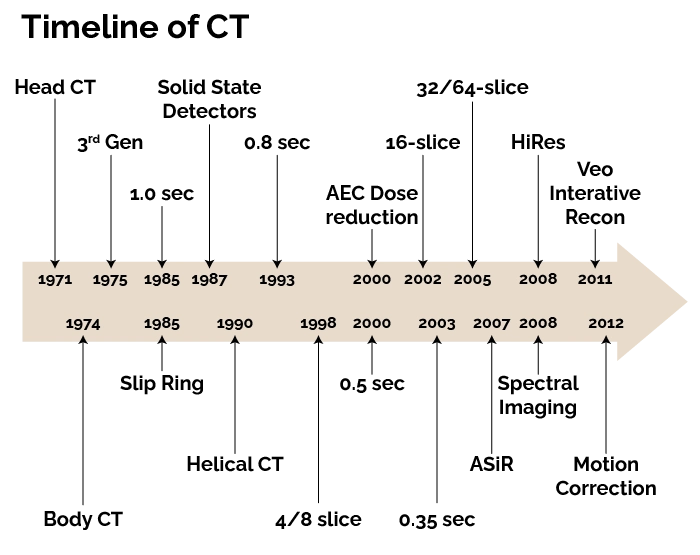
This section examines the key CT generations, each representing a significant advancement in scanning technology and diagnostic capabilities.
Hounsfield conceptually divided the brain into consecutive slices, like a loaf of bread. Then he planned to beam a series of X-rays through each layer, repeating this for each degree of a half-circle. The strength of each beam would be captured on the opposite side of the brain, with stronger beams indicating they had traveled through less dense material. (“50 years ago, the first CT scan let doctors see inside a living skull …”)
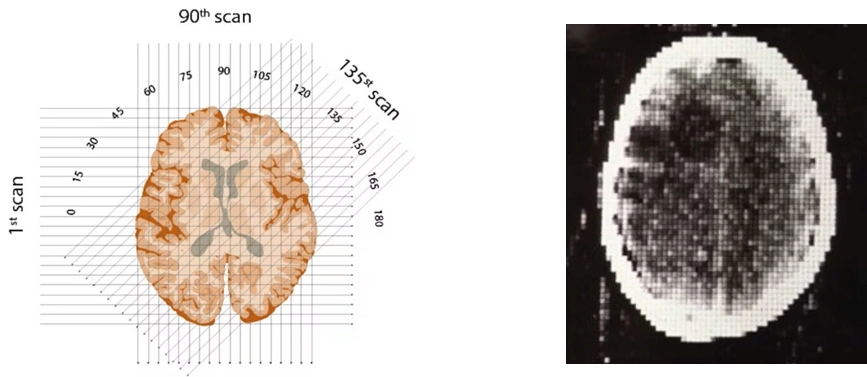 The first clinical CT scan showed a brain tumor visible as a darker blob. [‘Medical Imaging Systems: An Introductory Guide,’ Maier A, Steidl S, Christlein V, et al., editors.] www.ncbi.nlm.nih.gov [CC BY] creativecommons.org
The first clinical CT scan showed a brain tumor visible as a darker blob. [‘Medical Imaging Systems: An Introductory Guide,’ Maier A, Steidl S, Christlein V, et al., editors.] www.ncbi.nlm.nih.gov [CC BY] creativecommons.org On October 1, 1971, the team scanned their first patient: a middle-aged woman who showed signs of a brain tumor. It was not a fast process: 30 minutes for the scan, a drive across town with the magnetic tapes, 2.5 hours processing the data on an EMI mainframe computer, and capturing the image with a Polaroid camera before racing back to the hospital.
And there it was, in her left frontal lobe, a cystic mass about the size of a plum. With that, every other method of imaging the brain was obsolete.
In 1973, American Robert Ledley developed a whole-body scanner. This scanner could image other organs, blood vessels, and bones. It has become the hallmark of today’s medical imaging.
FIRST GENERATION
First-generation CT scanners, introduced in the early 1970s, are now considered old CT scan machines; they utilized a translate-rotate design with a pencil-thin X-ray beam and a single detector. In these systems, the X-ray tube and detector pair moved linearly across the patient to collect data along one projection, then rotated slightly around the patient and repeated the process. This sequential acquisition generated multiple projections that were later reconstructed into a single cross-sectional image. Because the system only captured one narrow beam at a time, scan times were lengthy, often taking several minutes per slice, and patient motion could easily degrade image quality. Despite these limitations, the technology provided unprecedented soft tissue contrast compared to conventional radiography, allowing visualization of brain structures and pathology that had previously been obscured.
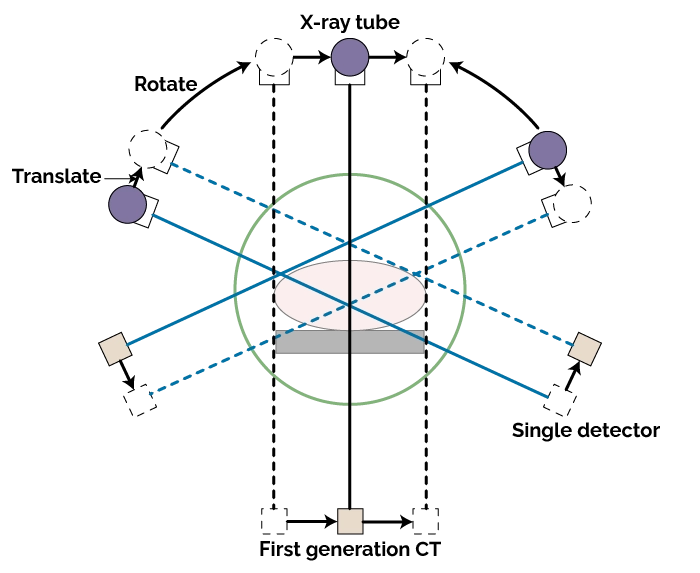 First-generation CT scanners emerged in the early 1970s and employed a “translate-rotate” design.
First-generation CT scanners emerged in the early 1970s and employed a “translate-rotate” design. Clinically, first-generation CT scanners were a breakthrough, particularly in neuroimaging. They were most commonly head-only units, as the system geometry and slow acquisition were impractical for larger body regions. Image matrix sizes were typically 80 × 80 or 128 × 128, which, though coarse by modern standards, offered revolutionary diagnostic information in conditions such as tumors, hemorrhage, and infarcts. Radiation doses were low because of the narrow beam and extended acquisition, but the long scan times limited their use in unstable patients. These early scanners paved the way for subsequent generations by proving the feasibility and diagnostic power of computed tomography, sparking rapid advancements in detector arrays and acquisition speed.
TAKE AWAY: translate-rotate, pencil beam.
SECOND GENERATION
Second-generation computed tomography scanners marked a significant advancement over their predecessors by adopting a narrow fan-shaped X-ray beam and a small array of detectors rather than a single pencil beam. The X-ray tube and detector array still performed a translate-rotate motion, but because the fan beam covered a wider section of the patient with each pass, fewer translation steps were required to acquire a full projection. This improvement reduced the total number of movements needed and thereby shortened acquisition time per slice, typically to under 20 seconds. The wider coverage also allowed for improved photon utilization and better signal-to-noise ratios, resulting in clearer images with fewer artifacts compared to first-generation systems.
 Second-generation CT scanners represented a significant leap in technology by employing a narrow fan-shaped X-ray beam and a detector array, replacing the single-detector pencil beam of earlier models.
Second-generation CT scanners represented a significant leap in technology by employing a narrow fan-shaped X-ray beam and a detector array, replacing the single-detector pencil beam of earlier models. Clinically, second-generation scanners expanded the utility of CT beyond solely head imaging, as the improved acquisition speed made it more feasible to scan other regions with acceptable motion tolerance. The fan-beam geometry allowed for increased detector efficiency, which translated into better spatial resolution and more reliable detection of soft tissue differences. Although still slower than later generations, these scanners offered a practical balance between image quality and acquisition time, making them invaluable for early whole-body computed tomography studies. Their development represented a key transitional step in CT evolution, setting the stage for third-generation rotate-rotate designs that would eventually dominate clinical practice.
TAKE AWAY: fan beam, faster acquisition.
THIRD GENERATION
Third-generation CT scanners introduced a rotate-rotate geometry, in which both the X-ray tube and a curved array of multiple detectors rotate together around the patient. Unlike the earlier translate-rotate designs, there is no linear translation step, allowing the system to collect a complete projection with each full rotation. This design significantly reduced scan times, often to just a few seconds per slice, and enabled continuous acquisition of data with far fewer mechanical movements. The use of a wide fan beam and hundreds of detectors improved photon capture and image quality, while also reducing motion artifacts that plagued earlier generations.
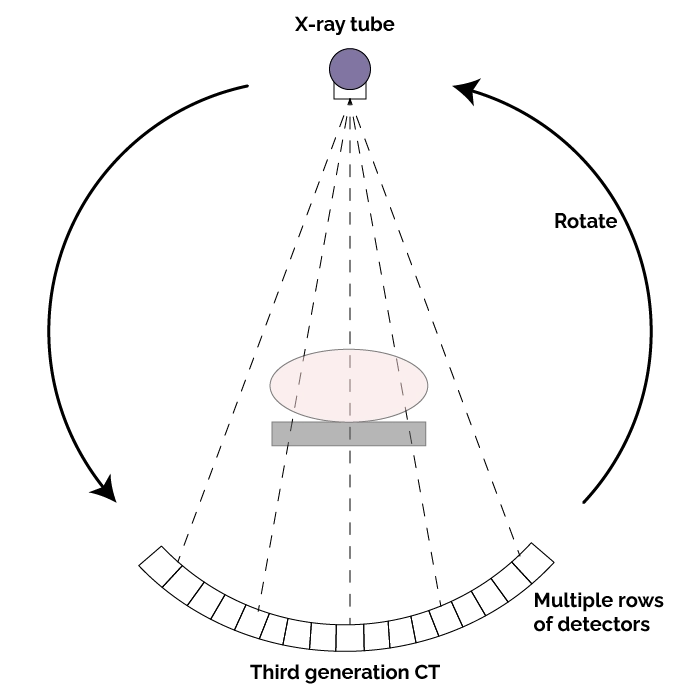 Third-generation CT scanners utilize a “rotate-rotate” geometry, where both the X-ray tube and a curved array of detectors rotate together around the patient.
Third-generation CT scanners utilize a “rotate-rotate” geometry, where both the X-ray tube and a curved array of detectors rotate together around the patient. From a clinical standpoint, third-generation scanners represented a major leap forward in versatility and diagnostic power. The rapid acquisition times allowed reliable imaging of not only the head but also the chest, abdomen, and extremities, making whole-body CT a routine diagnostic tool. The increased detector coverage and consistent geometry improved spatial resolution and reduced noise, supporting the detection of subtle lesions and vascular structures. These advancements directly contributed to faster workflow in emergency settings, enhanced patient throughput, and more accurate diagnostic capabilities, establishing the rotate-rotate design as the foundation for most modern CT systems.
TAKE AWAY: rotate-rotate geometry.
FOURTH GENERATION
Fourth-generation CT scanners introduced a rotate-stationary geometry, in which the X-ray tube rotates around the patient while a complete ring of detectors remains fixed in place. Instead of the detectors moving with the tube as in third-generation designs, thousands of stationary detectors encircle the gantry and continuously receive data as the tube rotates. This configuration eliminated the need for complex slip ring connections to a moving detector array and reduced mechanical wear, resulting in greater system durability and potentially more stable calibration over time. The design also allowed for very wide fan beams, improving coverage and reducing the total number of rotations needed for each scan.
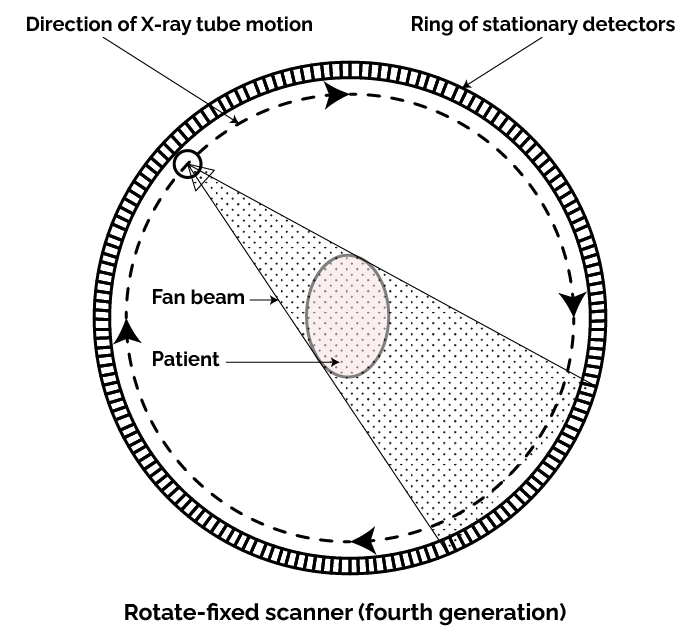 Fourth-generation CT scanners utilize a rotate–stationary geometry, where the X-ray tube rotates around the patient while a complete ring of detectors remains fixed.
Fourth-generation CT scanners utilize a rotate–stationary geometry, where the X-ray tube rotates around the patient while a complete ring of detectors remains fixed.Clinically, fourth-generation scanners offered fast acquisition times comparable to third-generation systems while providing improved image uniformity and reduced geometric distortions. Because the detector array was stationary, these systems could maintain precise alignment and consistent performance over prolonged use, which was particularly beneficial in high-volume settings. The increased speed and reliability made whole-body imaging more practical, and many units were optimized for specialized studies, including cardiac and vascular imaging. Although third-generation designs remained more common due to cost and complexity considerations, fourth-generation scanners demonstrated a significant evolution in computed tomography engineering and helped refine detector technology used in today’s advanced systems.
TAKE AWAY: stationary detectors, faster scans, increased cost, and complexity.
Helical (Spiral) CT
The advent of helical (spiral) CT in the 1990s revolutionized image acquisition by introducing slip ring technology, which allowed the X-ray tube and detectors to rotate continuously without the need for cables to rewind. This breakthrough enabled continuous data acquisition as the patient table moved through the gantry in a smooth, helical motion. The result was faster scans with reduced motion artifacts, allowing for enhanced visualization of dynamic structures. These capabilities improved vascular and thoracic imaging, as radiologists could capture entire regions during a single breath-hold, improving diagnostic accuracy in conditions such as pulmonary embolism or aortic dissection.
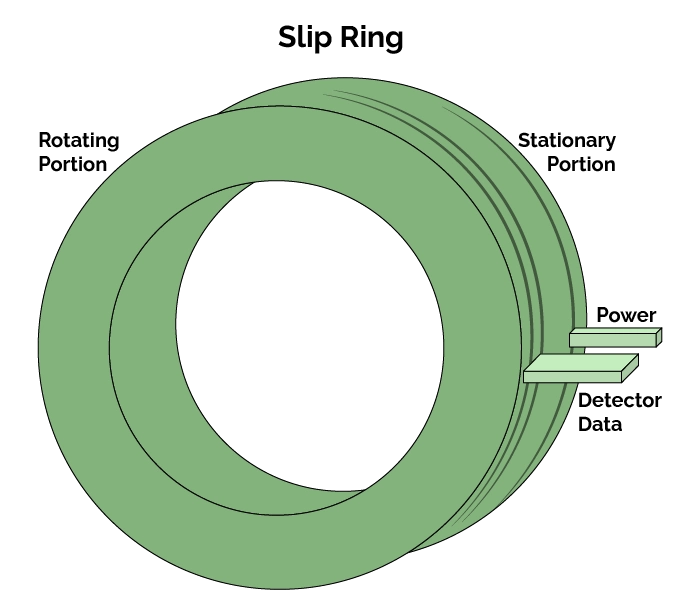 Helical (or spiral) CT utilizes slip-ring technology, enabling the X-ray tube and detectors to rotate continuously without the need for cable unwinding.
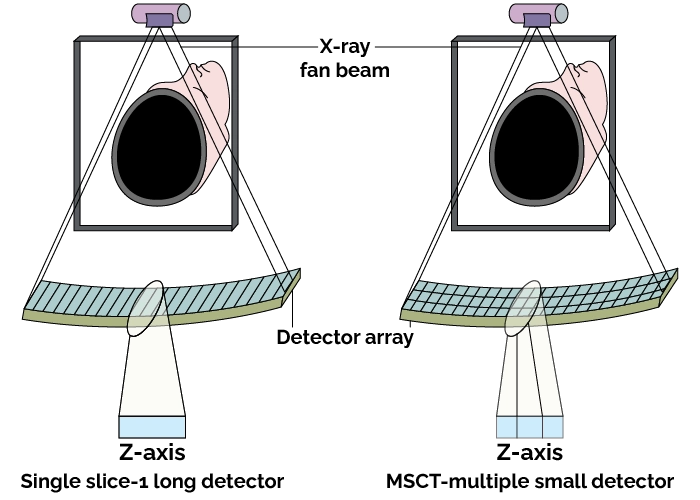
Helical (or spiral) CT utilizes slip-ring technology, enabling the X-ray tube and detectors to rotate continuously without the need for cable unwinding.Multidetector CT (MDCT)
Building on this foundation, multidetector CT (MDCT) emerged in the early 2000s, transitioning from single-row detectors to systems with 4, 16, 64, and now more than 320 slices per rotation. This evolution enabled sub-second whole-body imaging with dramatically improved spatial and temporal resolution. Clinically, MDCT has had a profound impact: cardiac CT angiography provides noninvasive coronary assessment, virtual colonoscopy offers a less invasive alternative for colorectal cancer screening, and lung nodule detection and follow-up have become faster and more reliable. Together, these innovations have transformed computed tomography into a versatile modality capable of high-speed, high-resolution imaging across multiple specialties.
Radiation Dose Awareness and Reduction
Modern CT imaging has placed strong emphasis on radiation dose optimization while maintaining diagnostic image quality. The guiding principle of what is known as ALARA, or As Low As Reasonably Achievable, underpins all computed tomography scanning protocols, ensuring that patients receive the minimum dose required to answer the clinical question. Technological advances such as automatic exposure control (AEC) dynamically adjust tube current based on patient size and anatomy, significantly lowering unnecessary exposure. In addition, iterative reconstruction techniques have revolutionized image processing by reducing noise and enhancing detail at lower radiation levels, allowing clinicians to confidently interpret high-quality images while minimizing patient risk.
Spectral (Dual-Energy) CT
Dual-energy CT (DECT) acquires data at two different X-ray energy levels, enabling unique tissue characterization beyond standard attenuation values. What this capability has done is allow radiologists to differentiate materials with similar appearances on conventional computed tomography, such as distinguishing uric acid from calcium in gout or performing iodine mapping to assess organ perfusion or tumor vascularity. In oncology, DECT aids in precise lesion characterization and treatment planning, while in cardiology, it improves plaque assessment and detection of myocardial defects. By providing virtual non-contrast images, DECT can also reduce the need for additional phases, further contributing to dose savings and comprehensive patient evaluation.
Artificial Intelligence and Deep Learning in CT Imaging
Artificial intelligence and deep learning algorithms are increasingly integrated into computed tomography workflows to enhance efficiency and accuracy in brain, spine, abdominal, whole-body scans, and more. Sophisticated models perform noise reduction during image reconstruction, producing clearer images at lower doses. Automated interpretation tools help detect critical findings such as intracranial hemorrhage, stroke, or pulmonary embolism in near real time, enabling rapid triage in emergency settings. These artificial intelligence computed tomography brain scans applications support faster triage and more accurate outcomes.
Beyond interpretation, AI assists with workflow optimization, selecting appropriate protocols based on clinical indications and patient factors, thereby reducing repeat scans and improving throughput. These advancements collectively elevate diagnostic confidence, streamline operations, and support safer, more personalized imaging.
Conclusion
Over recent history, CT scan technology has evolved from the first old, slow, brain-only, single-slice scanner machines to today’s rapid, multidetector systems enhanced by artificial intelligence and advanced reconstruction algorithms. Each generation introduced improvements in geometry, detector design, and computational power, leading to sharper images, shorter scan times, and more comprehensive diagnostic capabilities. Techniques such as iterative reconstruction, spectral imaging, and automatic exposure control have enabled significant dose reduction while preserving image quality, making computed tomography a cornerstone of modern medicine across neurology, oncology, cardiology, and trauma care.
Despite these achievements, ongoing challenges remain. There is a continued need to reduce radiation dose further, ensure equitable access to cutting-edge computed tomography technology in resource-limited settings, and seamlessly integrate artificial intelligence tools into clinical practice for the investigation of brain, spine, chest, abdomen, pelvis, and more. Looking forward, photon-counting detectors, ultra-high-resolution imaging, and real-time functional techniques promise to push CT into new frontiers, supporting precision medicine and advancing population health initiatives. With these innovations, CT is poised to remain an indispensable tool, combining diagnostic power with ever-increasing safety and efficiency.
References
- Petrik V, Apok V, Britton JA, Bell BA, Papadopoulos MC. Godfrey Hounsfield and the dawn of computed tomography. Neurosurgery. 2006 Apr;58(4):780-7; discussion 780-7. PubMed
- Bhattacharyya KB. Godfrey Newbold Hounsfield (1919-2004): The man who revolutionized neuroimaging. Ann Indian Acad Neurol. 2016 Oct-Dec;19(4):448-450. PMC free article PubMed
- Tan SY, Poole PS. Allan MacLeod Cormack (1924-1998): Discoverer of computerized axial tomography. Singapore Med J. 2020 Jan;61(1):4-5. PMC free article PubMed
- National Institute of Biomedical Imaging and Bioengineering: Computed Tomography (CT)
- The Conversation: 50 years ago, the first CT scan let doctors see inside a living skull
- Mayo Clinic: CT scan
- TeachMeAnatomy: Computed Tomography (CT) Scans
- CDC: CT scans facts and stats
- NCBI Bookshelf: Computed Tomography
- Raju TN. The Nobel chronicles. 1979: Allan MacLeod Cormack (b 1924); and Sir Godfrey Newbold Hounsfield (b 1919). Lancet. 1999 Nov 06;354(9190):1653. PubMed
- Willemink, M. J., & Persson, M. (2021). Photon-counting CT: technical principles and clinical prospects. Radiology, 299(2), 334-351. https://doi.org/10.1148/radiol.2021203451
- Willemink, M. J., & Noël, P. B. (2019). The evolution of image reconstruction for CT-from filtered back projection to artificial intelligence. European Radiology, 29(5), 2185-2195. https://doi.org/10.1007/s00330-018-5810-7
- Willemink, M. J., & Noël, P. B. (2021). The future of image reconstruction in CT: AI-driven, photon-counting, and beyond. European Radiology Experimental, 5(1), 6. https://doi.org/10.1186/s41747-020-00185-0
- O’Connor, S. D., & Sodickson, A. D. (2020). Artificial intelligence in radiology: current applications and future directions. Radiologic Clinics of North America, 58(6), 1043-1052. https://doi.org/10.1016/j.rcl.2020.06.004
- McCollough, C. H., Leng, S., Yu, L., & Fletcher, J. G. (2020). Dual- and multi-energy CT: principles, technical approaches, and clinical applications. Radiology, 297(3), 640-657. https://doi.org/10.1148/radiol.2020192446
- Rossi, A., Dwivedi, A., Jabbour, A., Naoum, C., Bax, J. J., & Sharma, R. K. (2021). Cardiac CT in 2021: Current status and future directions. Journal of Cardiovascular Computed Tomography, 15(2), 108-119. https://doi.org/10.1016/j.jcct.2020.09.007
Image Sources
- Life in the Fast Lane: Godfrey Hounsfield
- The Conversation image source: EMI scanner
- The Conversation image source
- The Conversation image source
Disclaimer: The information provided on this website is intended to provide useful information to radiologic technologists. This information should not replace information provided by state, federal, or professional regulatory and authoritative bodies in the radiological technology industry. While Medical Professionals strives to always provide up-to-date and accurate information, laws, regulations, statutes, rules, and requirements may vary from one state to another and may change. Use of this information is entirely voluntary, and users should always refer to official regulatory bodies before acting on information. Users assume the entire risk as to the results of using the information provided, and in no event shall Medical Professionals be held liable for any direct, consequential, incidental or indirect damages suffered in the course of using the information provided. Medical Professionals hereby disclaims any responsibility for the consequences of any action(s) taken by any user as a result of using the information provided. Users hereby agree not to take action against, or seek to hold, or hold liable, Medical Professionals for the user’s use of the information provided.